
If you are involved with transportation, it is likely that you learned about the “3 E’s of safety” – Education, Enforcement and Engineering. It sounds logical, surely you need those three things. But whether through study or lived experience it becomes obvious that education and enforcement are inadequate in response to road designs that encourage speeding and the increasing size and weight of vehicles. We can tell people all day to “slow down”, but that doesn’t do much when the built environment is saying “go fast”. Indeed, calls to wear bright clothing or carry a flashlight start to sound like an evasion of responsibility by the people with the power and ability to design roads and vehicles to ensure safe outcomes.
Thus entered the “Safe Systems Approach” with its commendable attempt to provide greater clarity on how to achieve safety, and its exhortation for design to recognize that humans can make mistakes. Unfortunately, the 3 E’s crowd can still shoehorn the old conceptual approach into the Safe Systems Approach, which calls for Safer Roads, Safer Vehicles, Safer People and Safer Speeds.
So how to prioritize interventions? The “Safe Systems Pyramid” (sounds similar but is radically different) – takes an epidemiological approach to identify the agent of disease.
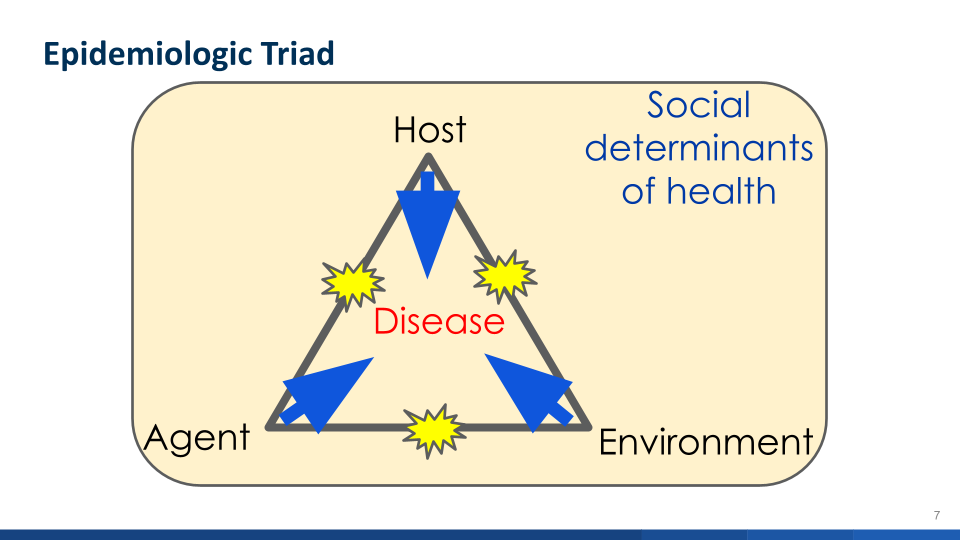
Presenter Dr. Dave Ederer, who co-authored the groundbreaking paper on the Pyramid, discussed malaria as an example. Malaria is the agent and it is spread by mosquitoes. To disrupt the spread you can separate people from mosquitos and you can change the environment by removing standing water in which mosquitos breed.
For traffic safety the agent is energy (the speed and mass of vehicles) impacting upon fragile human bodies. That’s what kills people. As tempting as it is to blame inattention or allegedly poor clothing choices, those individual choices go to how the cause of death reaches the host, it is not the agent. When you know the disease you can start thinking rationally about how to disrupt its spread to people and in the environment. For example, the three point seat belt physically prevents heads from hitting dashboards and we have wisely required it in all vehicles. It disrupts the chain of causation.
The health profession also relies on the health impact pyramid, which prioritizes action by examining different approaches and ranking them. Something similar can be found in OSHA’s hierarchy of controls.
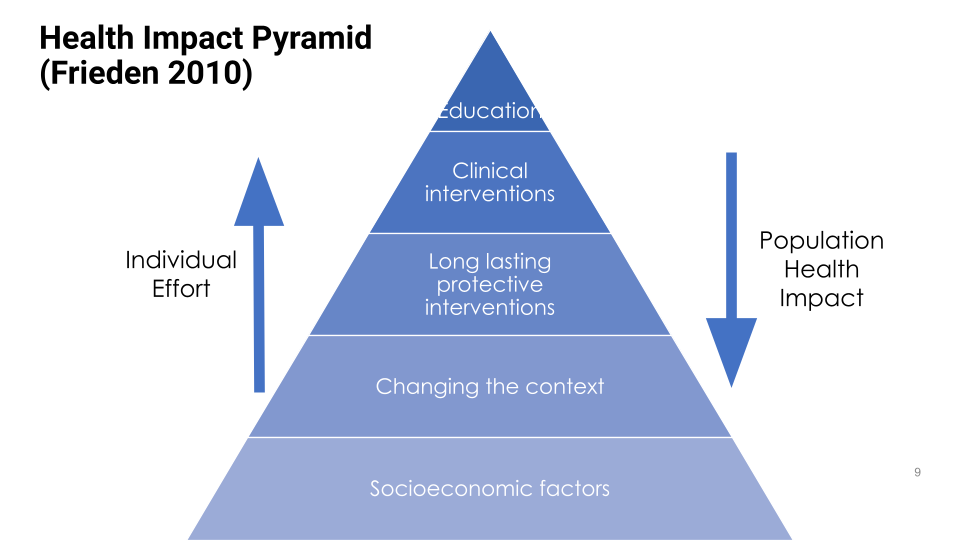
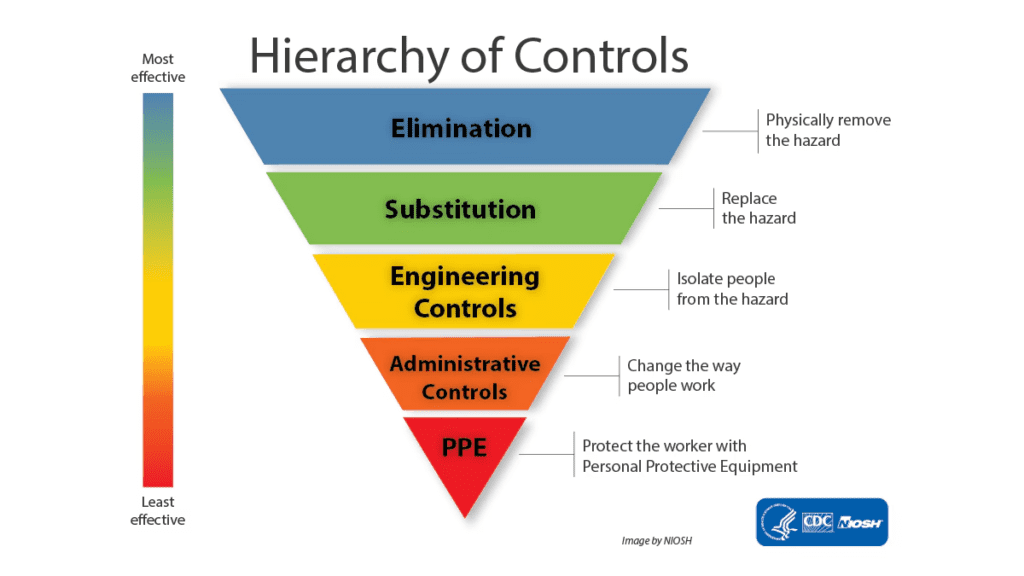
Not surprisingly, education, or administrative controls (rules) are the least effective interventions. They require lots of people to make the right choices, sometimes against their own analysis in the moment. (“I can sneak a look at the text message” or “that crosswalk is too far away, I can cross here.”) In contrast, actions that separate the agent and host, take no individual effort, and are “always on” have the greatest impact. Imagine housing close to your destinations with street design compelling slow vehicle speeds.
Put it all together, and we have the Safe Systems Pyramid
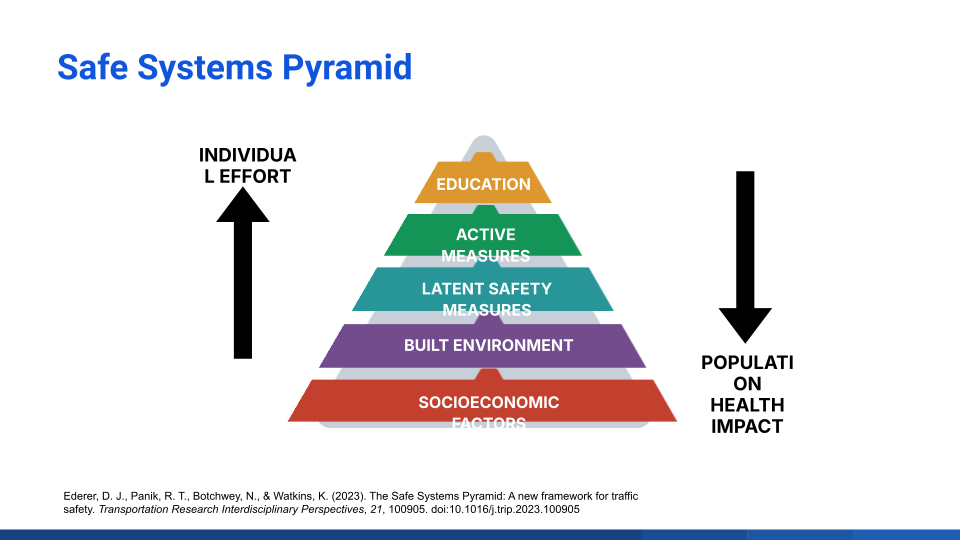
We’ve already discussed education, so let’s look at each level for other examples
| Active measures | Seat belts are active because you have to take action each time. |
| Latent Safety Measures | Crumple zone in your vehicle, or a bollard on the roadway edge, are “always on”. |
| Built environment | Roadway design to reduce speeds. |
| Socioeconomic factors | Place jobs, retails schools and housing close enough to each other to reduce time on the road. It is “always on” and has a broad population impact. |
With this approach, you can identify how other interventions fit into the Safe Systems Pyramid. A broad spectrum of safety professionals and advocates are now urging transportation agencies to formally adopt the Safe Systems Pyramid.
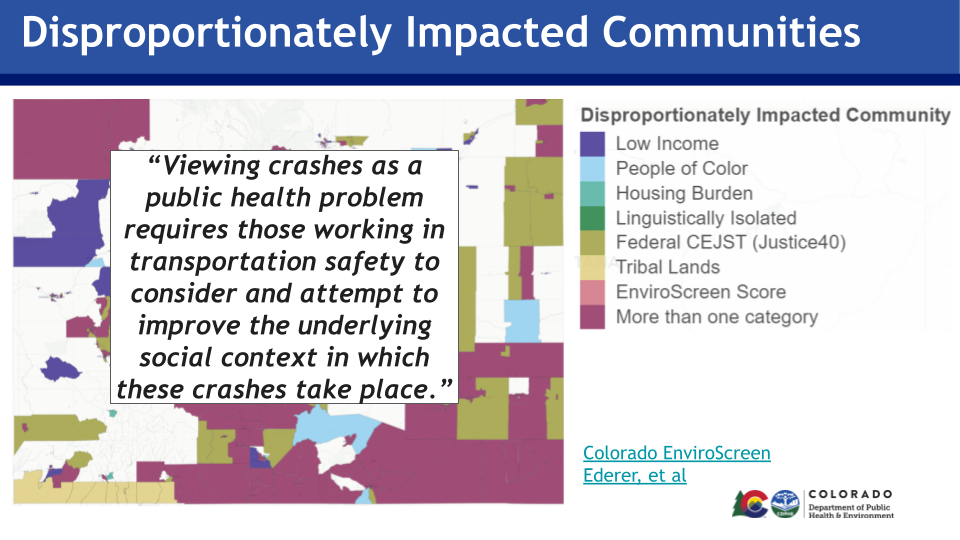
The next webinar presenter, Steph Leonard, is currently working to implement the Pyramid across state agencies in Colorado, including public health and transportation departments. She presented how Colorado uses the Pyramid to look at the underlying social context in which crashes take place, identify where injuries occur, and support appropriate interventions.
Some other observations from the webinar
It turns out that CDC once had an engineering department and the CDC’s first director was an engineer. Somehow, that link between public health and engineering has been lost even though historically that link was strong. Consider how engineers had a central role in building clean water, sewer, and stormwater systems. Dave urged transportation engineers and public health professionals to renew that connection.
Dave also pointed out how we do not currently treat traffic crashes in the same way as other public health emergencies. For example, if the public health department discovers listeria on meat in the supermarket, it removes it. To put traffic calming on the street, it might require a law, public hearings, community buy-in, or more. In Dave’s words we don’t hold a public hearing on “How do you feel about listeria? Should we have that in our deli meat?”
The webinar was made possible by the Centers for Disease Control and Prevention’s Active People, Healthy Nation campaign, which is aimed at increasing physical activity and improving health and quality of life.